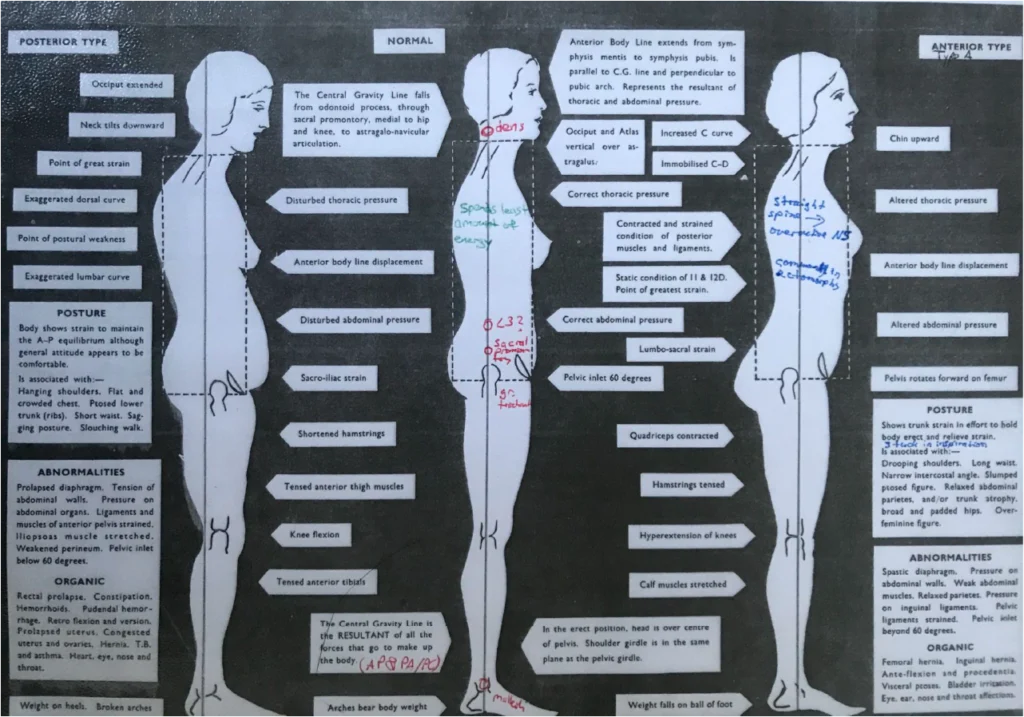
Osteopaths consider two different types of posture – an anterior type, where the centre of gravity line has moved anteriorly, and a posterior type, where the centre of gravity line (CGL) has moved posteriorly.
(Here are notes from my student days at the European School of Osteopathy. I could not find satisfying images on the internet, so I apologise that some of my writing is not easily readable. I must credit John Wernham, from whom the diagrams stem.)
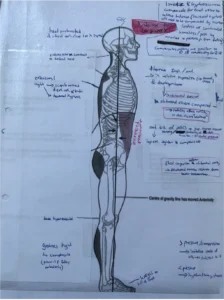
Anterior type (with anterior pelvic tilt):
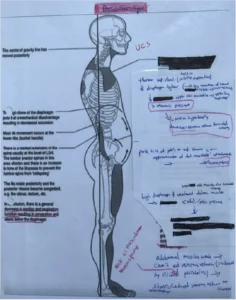
Posterior type (with upper crossed syndrome and posterior pelvic tilt):
Meanwhile, sedentary work often results in two main body positions:
1. anterior pelvic tilt
2. upper crossed syndrome (internally rotated and protracted shoulders)
An anterior pelvic tilt is associated with the anterior type of posture, while upper crossed syndrome is a posterior type.
Often individuals are a combination of anterior and posterior types, e.g. posterior in the upper half of the body, and anterior in the lower half.
This is because the body will try to compensate.